X Post by @NHSMillions: A Critique
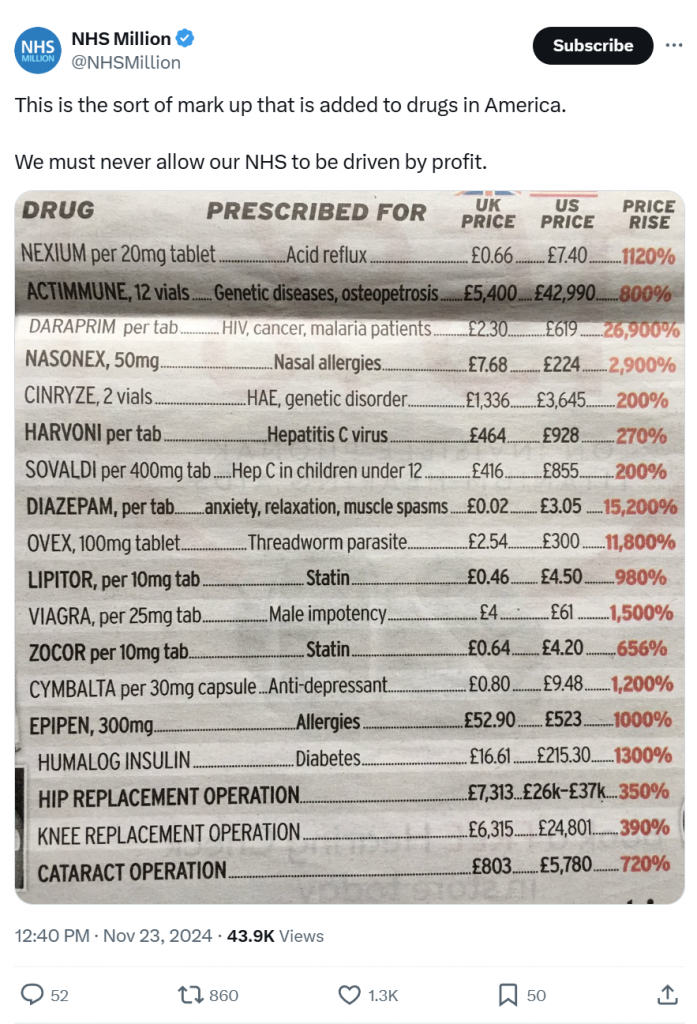
This post was published by the account @NHSMillions at 12:40 PM on Nov 23, 2024.
Critique of the Article and Image
The image used in the X post was found in a post on the following linked website:
Context and Timeliness
The article, published in 2019, reflects the pre-Brexit fears of a potential U.S.-UK trade deal involving the NHS. It discusses concerns about drug pricing and privatization, using the table to highlight disparities in drug and healthcare costs between the UK and the U.S. While these fears were valid at the time, much of the debate has since shifted. Brexit has occurred, and no significant trade deal with the U.S. involving the NHS has materialized. This diminishes the table’s immediate relevance in the current political and healthcare landscape.
Data Source and Presentation
The table in the article lacks attribution to a credible, independent source. Without a citation, the accuracy and methodology behind these figures remain unverified, leaving the reader to question whether the price disparities are representative of real-world averages or cherry-picked examples. Furthermore, the table simplifies complex pricing structures, omitting factors such as insurance coverage, rebates, government negotiations, and differences in healthcare systems.
Limitations of the Data
- Selective Comparison: The table compares UK prices, heavily influenced by NHS-negotiated contracts, with U.S. prices from a predominantly private healthcare market. It fails to account for factors such as different funding models, pharmaceutical pricing policies, and patient outcomes. These differences make direct price comparisons misleading.
- Outdated Focus: The table primarily addresses the cost of drugs and procedures. However, healthcare privatization involves broader issues, such as service access, funding cuts, and operational inefficiencies. The focus on pharmaceuticals risks reducing a systemic debate to isolated examples.
- Inflammatory Tone: The table’s percentage increases are dramatic, suggesting extreme exploitation in the U.S. healthcare system. While highlighting disparities is important, the table does not delve into why such disparities exist or whether they are representative of broader trends. This oversimplified presentation may foster sensationalism rather than nuanced understanding.
- Pre-Brexit Lens: The fears articulated in 2019 about U.S. influence on the NHS under a post-Brexit trade deal were speculative. Four years later, no evidence has emerged of NHS privatization or American pharmaceutical companies dominating UK healthcare. This undermines the argument’s relevance to today’s realities.
Implications for Today’s Audience
While the article served as a cautionary piece during pre-Brexit debates, its assumptions should now be revisited. Healthcare funding and privatization remain pressing concerns in the UK, but they are shaped more by internal government policies than by external trade deals. The ongoing debate about NHS sustainability, staffing shortages, and operational efficiency in a post-pandemic world has superseded concerns about U.S. influence.
Recommendations for Improved Analysis
To foster a more informed discussion:
- Update the Data: Use recent, transparent sources to highlight any ongoing price disparities. Reflect on post-Brexit policy developments and their impact on NHS funding and privatization risks.
- Provide Context: Explain why prices differ between countries, considering pharmaceutical regulations, healthcare funding models, and market dynamics.
- Broaden the Scope: Address systemic factors, such as workforce challenges, infrastructure pressures, and public satisfaction, rather than isolating pharmaceutical costs.
- Focus on Current Risks: Emphasize pressing issues like NHS underfunding and privatization creep through outsourcing, rather than speculative fears about U.S. influence.
Conclusion
The article and table serve as a snapshot of pre-Brexit fears but are largely outdated in today’s context. The discussion on NHS privatization should now center on domestic policy decisions, grounded in current data and real-world impacts. By focusing on internal challenges and avoiding overly simplistic comparisons, the debate can remain relevant and constructive for safeguarding the NHS.